Bursitis Foot Pain Signs And Symptoms
Overview
Between the heel bone and the plantar fascia is a small fluid filled sac that is called the plantar (bottom of) calcaneal (heel bone) bursa. The plantar calcaneal bursa?s job is to allow the plantar fascia to glide easily over the heel bone without irritation. If this becomes inflamed and irritated a plantar calcaneal bursitis occurs which can be extremely painful and disabling forcing the athlete to stop training.
Causes
Repetitive overuse injury of the ankle during long periods of running and or walking. Tight shoes. The heel counter of the shoe constantly rubbing against the back of the heel. Wearing shoes with a low cut heel counter. Abnormal foot mechanics (abnormal pronation). Poor flexibility. Inappropriate training.
Symptoms
Retrocalcaneal bursitis is very similar to Achilles bursitis as the bursae are very close in proximity and symptoms are almost identical however retrocalcaneal bursitis is a lot more common. The symptoms of bursitis vary depending on whether the bursitis is the result of injury or an underlying health condition or from infection. From normal overuse and injury the pain is normally a constant dull ache or burning pain at the back of the heel that is aggravated by any touch, pressure like tight shoes or movement of the joint. There will normally be notable swelling around the back of the heel. In other cases where the bursa lies deep under the skin in the hip or shoulder, swelling might not be visible. Movement of the ankle and foot will be stiff, especially in the mornings and after any activity involving the elbow. All of these symptoms are experienced with septic bursitis with the addition of a high temperature of 38?C or over and feverish chills. The skin around the affected joint will also appear to be red and will feel incredibly warm to the touch. In cases of septic bursitis it is important that you seek medical attention. With injury induced bursitis if symptoms are still persisting after 2 weeks then report to your GP.
Diagnosis
When a patient has pain in a joint, a careful physical examination is needed to determine what type of movement is affected and if there is any swelling present. Bursitis will not show up on x-rays, although sometimes there are also calcium deposits in the joint that can be seen. Inserting a thin needle into the affected bursa and removing (aspirating) some of the synovial fluid for examination can confirm the diagnosis. In most cases, the fluid will not be clear. It can be tested for the presence of microorganisms, which would indicate an infection, and crystals, which could indicate gout. In instances where the diagnosis is difficult, a local anesthetic (a drug that numbs the area) is injected into the painful spot. If the discomfort stops temporarily, then bursitis is probably the correct diagnosis.
Non Surgical Treatment
Treatment is primarily comprised of relief from the painful activity (running). It is important that shoes do not pinch the heel. If satisfactory progress is not made during the rehabilitation, medical treatment can be considered in the form of rheumatic medicine (NSAID) or injection of corticosteroid in the bursa. Injections should be performed under ultrasound guidance to ensure optimal effect and reduce the risk of injecting into the Achilles itself. If progress is not made neither through rehabilitation nor medicinal treatment, surgical treatment can be attempted.
Surgical Treatment
Surgery is rarely done strictly for treatment of a bursitis. If any underlying cause is the reason, this may be addressed surgically. During surgery for other conditions, a bursa may be seen and removed surgically.
Between the heel bone and the plantar fascia is a small fluid filled sac that is called the plantar (bottom of) calcaneal (heel bone) bursa. The plantar calcaneal bursa?s job is to allow the plantar fascia to glide easily over the heel bone without irritation. If this becomes inflamed and irritated a plantar calcaneal bursitis occurs which can be extremely painful and disabling forcing the athlete to stop training.
Causes
Repetitive overuse injury of the ankle during long periods of running and or walking. Tight shoes. The heel counter of the shoe constantly rubbing against the back of the heel. Wearing shoes with a low cut heel counter. Abnormal foot mechanics (abnormal pronation). Poor flexibility. Inappropriate training.
Symptoms
Retrocalcaneal bursitis is very similar to Achilles bursitis as the bursae are very close in proximity and symptoms are almost identical however retrocalcaneal bursitis is a lot more common. The symptoms of bursitis vary depending on whether the bursitis is the result of injury or an underlying health condition or from infection. From normal overuse and injury the pain is normally a constant dull ache or burning pain at the back of the heel that is aggravated by any touch, pressure like tight shoes or movement of the joint. There will normally be notable swelling around the back of the heel. In other cases where the bursa lies deep under the skin in the hip or shoulder, swelling might not be visible. Movement of the ankle and foot will be stiff, especially in the mornings and after any activity involving the elbow. All of these symptoms are experienced with septic bursitis with the addition of a high temperature of 38?C or over and feverish chills. The skin around the affected joint will also appear to be red and will feel incredibly warm to the touch. In cases of septic bursitis it is important that you seek medical attention. With injury induced bursitis if symptoms are still persisting after 2 weeks then report to your GP.
Diagnosis
When a patient has pain in a joint, a careful physical examination is needed to determine what type of movement is affected and if there is any swelling present. Bursitis will not show up on x-rays, although sometimes there are also calcium deposits in the joint that can be seen. Inserting a thin needle into the affected bursa and removing (aspirating) some of the synovial fluid for examination can confirm the diagnosis. In most cases, the fluid will not be clear. It can be tested for the presence of microorganisms, which would indicate an infection, and crystals, which could indicate gout. In instances where the diagnosis is difficult, a local anesthetic (a drug that numbs the area) is injected into the painful spot. If the discomfort stops temporarily, then bursitis is probably the correct diagnosis.
Non Surgical Treatment
Treatment is primarily comprised of relief from the painful activity (running). It is important that shoes do not pinch the heel. If satisfactory progress is not made during the rehabilitation, medical treatment can be considered in the form of rheumatic medicine (NSAID) or injection of corticosteroid in the bursa. Injections should be performed under ultrasound guidance to ensure optimal effect and reduce the risk of injecting into the Achilles itself. If progress is not made neither through rehabilitation nor medicinal treatment, surgical treatment can be attempted.
Surgical Treatment
Surgery is rarely done strictly for treatment of a bursitis. If any underlying cause is the reason, this may be addressed surgically. During surgery for other conditions, a bursa may be seen and removed surgically.
How To Alleviate Hammertoe Pain
 Overview
Overview
hammertoes a bending and hardening of the joints of the second, third, fourth, or fifth toes. If you look down at your feet and you can?t see the tips of the toenails, you might suffer from hammertoe. Early signs of hammertoe are a bend in the joint of any toe except the big toe. The bend in the joint causes the top of the toe to appear to curl under as if it?s ?hammering? into the floor.
Causes
Poorly fitting shoes and muscle imbalances are the most common causes of hammertoe. When shoes are too narrow or do not accommodate the shape and size of your feet, they often contort the position of your toes. Choosing a shoe that fits is very important when it comes to avoiding foot problems like bunions or hammertoe. Having your toes bent for an extended period of time in a shoe that is too narrow or small forces your toes to adapt to the cramped space. With time, the muscles in your feet become accustomed to holding the flexed position of your toes, making it harder, or even impossible to straighten them.
 Symptoms
Symptoms
People with a hammer toe will often find that a corn or callus will develop on the top of the toe, where it rubs against the top of the footwear. This can be painful when pressure is applied or when anything rubs on it. The affected joint may also be painful and appear swollen.
Diagnosis
Although hammertoes are readily apparent, to arrive at a diagnosis the foot and ankle surgeon will obtain a thorough history of your symptoms and examine your foot. During the physical examination, the doctor may attempt to reproduce your symptoms by manipulating your foot and will study the contractures of the toes. In addition, the foot and ankle surgeon may take x-rays to determine the degree of the deformities and assess any changes that may have occurred.
Non Surgical Treatment
A toe doctor can provide you with devices such as hammer toe regulators or straighteners. These are also available for purchase locally. Another good idea is to start the hammer toe rehabilitation process by gently trying to straighten the joint and moving and flexing the affected toe as much as possible without straining it. If hammer toe taping doesn?t work, you may require surgery. If the joints and tendons have stiffened to a point of non-movement, hammer toe corrective surgery may need to enter the toe and either cut or manually move some of the tendons and ligaments. Although the treatment is relatively safe fast, you may deal with some stiffness afterwards.
Surgical Treatment
Hammer toe can be corrected by surgery if hammertoes conservative measures fail. Usually, surgery is done on an outpatient basis with a local anesthetic. The actual procedure will depend on the type and extent of the deformity. After the surgery, there may be some stiffness, swelling and redness and the toe may be slightly longer or shorter than before. You will be able to walk, but should not plan any long hikes while the toe heals, and should keep your foot elevated as much as possible.
 Prevention
Prevention
As you get older, feet get bigger. Get your feet measured every time you buy shoes. Don't go by shoe sizes. Shoe sizes vary among manufacturers; a shoe is the right size only when it fits comfortably. The ball of your foot should fit into the widest part of the shoe. A shoe should be sturdy such that it only bends in the ball of the foot, exactly where your big toes bend. Any shoe that can be bent anywhere along the sole or twisted side to side is generally too flimsy.
Hammer Toe Treatment Pain
 Overview
Overview
A hammertoe is a toe that is bent because of a weakened muscle. The weakened muscle makes the tendons (tissues that connect muscles to bone) shorter, causing the toes to curl under the feet. Hammertoes can run in families. They can also be caused by shoes that are hammertoes too short. Hammertoes can cause problems with walking and can lead to other foot problems, such as blisters, calluses, and sores. Splinting and corrective footwear can help in treating hammertoes. In severe cases, surgery to straighten the toe may be necessary.
Causes
Hammer toes are most frequently caused by a muscle - tendon imbalance in the foot, and are seen both in adults and children. Foot muscles work in pairs to straighten and bend the toes. If your foot has a biomechanical defect, the muscles tighten and the tendons shorten. Eventually, the toe muscles can?t straighten the toe, even when barefoot. Contributing factors are poor choices in footwear, arthritis, or trauma.
 Symptoms
Symptoms
If the toes remain in the hammertoe position for long periods, the tendons on the top of the foot will tighten over time because they are not stretched to their full length. Eventually, the tendons shorten enough that the toe stays bent, even when shoes are not being worn. The symptoms of hammertoe include a curling toe, pain or discomfort in the toes and ball of the foot or the front of the leg, especially when toes are stretched downward, thickening of the skin above or below the affected toe with the formation of corns or calluses, difficulty finding shoes that fit well. In its early stages, hammertoe is not obvious. Frequently, hammertoe does not cause any symptoms except for the claw-like toe shape.
Diagnosis
Most health care professionals can diagnose hammertoe simply by examining your toes and feet. X-rays of the feet are not needed to diagnose hammertoe, but they may be useful to look for signs of some types of arthritis (such as rheumatoid arthritis) or other disorders that can cause hammertoe.
Non Surgical Treatment
Putting padding between your toes and strapping them in place can help to stop pain caused by the toes rubbing. Custom-made insoles for your shoes will help to take the pressure off any painful areas. Special shoes that are wider and deeper than normal can stop your toes rubbing. However if your pain persists your consultant may recommend an surgery.
Surgical Treatment
If pinning the toe is not required during the procedure, then the surgery could be preformed in the doctor's office under a local anesthesia. Some patients prefer the comfort of sedation during the surgery and if this is the case or if a pin must be placed, then the surgery could be preformed in an outpatient surgery center.
Everything You Want To Know About Bunions
Overview
 A bunion (a.k.a Hallux Valgus) is a common foot condition associated with a prominent bump on the inside of the forefoot (see Figure 1). The word bunion? comes from the Greek root for the word turnip. Bunions can lead to discomfort over the prominence, especially if patients wear tight fitting shoes. It is common for bunions to run in family? and gradually increase over time. The vast majority of bunions can be managed successfully with basic non-operative treatment. Surgery is reserved for patients who have persistent symptoms in spite of appropriate non-operative treatment.
A bunion (a.k.a Hallux Valgus) is a common foot condition associated with a prominent bump on the inside of the forefoot (see Figure 1). The word bunion? comes from the Greek root for the word turnip. Bunions can lead to discomfort over the prominence, especially if patients wear tight fitting shoes. It is common for bunions to run in family? and gradually increase over time. The vast majority of bunions can be managed successfully with basic non-operative treatment. Surgery is reserved for patients who have persistent symptoms in spite of appropriate non-operative treatment.
Causes
Despite the popular belief, wearing high heels and too-narrow shoes does not cause bunions. Wearing them can irritate, aggravate, or accelerate the formation of the bunion, but are not the root cause. Bunions are more commonly inherited, if your parents or grandparents had bunions, you may also get one. Bunions can also be caused by trauma or injury to the joints, ligaments, or bones of the foot.
Symptoms
The most common symptoms of foot bunions are toe Position, the toe points inwards towards the other toes in the foot into the hallux adbucto valgus position and may even cross over the next toe. Bony Lump, swelling on the outer side of the base of the toe which protrudes outwards. Redness, over the bony lump where it becomes inflamed. Hard Skin, over the bony lump known as a callus. Pain, it is often painful around the big toe, made worse by pressure on the toe and weight bearing activities. Change in Foot Shape, Your whole foot may gradually change shape for example getting wider. Stiffness, the big toe often becomes stiff and may develop arthritis. Foot bunions are more common with increasing age. They develop gradually overtime from repeated force through the big toe and left untreated, become more pronounced with worsening symptoms.
Diagnosis
Bunions are readily apparent - the prominence is visible at the base of the big toe or side of the foot. However, to fully evaluate the condition, the foot and ankle surgeon may take x-rays to determine the degree of the deformity and assess the changes that have occurred. Because bunions are progressive, they don?t go away, and will usually get worse over time. But not all cases are alike - some bunions progress more rapidly than others. Once your surgeon has evaluated your bunion, a treatment plan can be developed that is suited to your needs.
Non Surgical Treatment
Treatment may be surgical or non-surgical. The goal of non-surgical treatment is to relieve pressure on the foot and to prevent pressure sores and foot ulcers. This is accomplished by prescribing accommodative shoes with a wide toe box - sandals or extra depth shoes with soft moulded insoles. It may also be possible to relax the leather on shoes to make room for a bunion. 
Surgical Treatment
In cases where joint pain and deformity are severe, joint replacement surgery may be recommended. This may particularly be recommended when arthritis is present in the joint. Surgery may be carried out under a local, regional or general anaesthetic. Most cases are performed as a day stay procedure. However, an overnight stay in hospital may be required if the surgery is more extensive. The type of surgery to be performed, the type of anaesthetic to be used and the expected hospital stay should be discussed with your surgeon prior to surgery.
Prevention
Because bunions develop slowly, taking care of your feet during childhood and early adulthood can pay off later in life. Keep track of the shape of your feet as they develop over time, especially if foot problems run in your family. Exercising your feet can strengthen them. Learn to pick up small objects, like a pencil or pebble, with your toes. Wear shoes that fit properly and don't cramp or pinch your toes. Women should avoid shoes with very high heels or pointed toes.
Overpronation Of The Feet
Overview
Over-pronation is very common and affects millions of people. To better understand this condition, we'll take a closer look at the 3 most common foot types. An estimated 70% of the population has fallen arches (or a low arch). Only 20% has a normal arch. And 10% have abnormal feet, in other words they either have flat feet or the opposite a high arched foot.
Causes
Over-pronation is very prominent in people who have flexible, flat feet. The framework of the foot begins to collapse, causing the foot to flatten and adding additional stress to other parts of the foot. Therefore over-pronation can often lead to a case of Plantar Fasciitis, Heel Spurs, Metatarsalgia, Post-tib Tendonitis and/or Bunions. There are many causes of flat feet. Obesity, pregnancy or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. People with flat feet often do not experience discomfort immediately, and some never suffer from any discomfort at all. However, when symptoms develop and become painful, walking becomes awkward and causes increased strain on the feet and calves.
Symptoms
When standing, your heels lean inward. When standing, one or both of your knee caps turn inward. Conditions such as a flat feet or bunions may occur. You develop knee pain when you are active or involved in athletics. The knee pain slowly goes away when you rest. You abnormally wear out the soles and heels of your shoes very quickly.
Diagnosis
If you cannot afford to get a proper gait analysis completed, having someone observe you on a treadmill from behind will give you an idea if you are an overpronator. It is possible to tell without observing directly whether you are likely to be an overpronator by looking at your foot arches. Check your foot arch height by standing in water and then on a wet floor or piece of paper which will show your footprint. If your footprints show little to no narrowing in the middle, then you have flat feet or fallen arches. This makes it highly likely that you will overpronate to some degree when running. If you have low or fallen arches, you should get your gait checked to see how much you overpronate, and whether you need to take steps to reduce the level to which you overpronate. Another good test is to have a look at the wear pattern on an old pair of trainers. Overpronators will wear out the outside of the heel and the inside of the toe more quickly than other parts of the shoe. If the wear is quite even, you are likely to have a neutral running gait. Wear primarily down the outside edge means that you are a supinator. When you replace your running shoes you may benefit from shoes for overpronation. Motion control or stability running shoes are usually the best bet to deal with overpronation.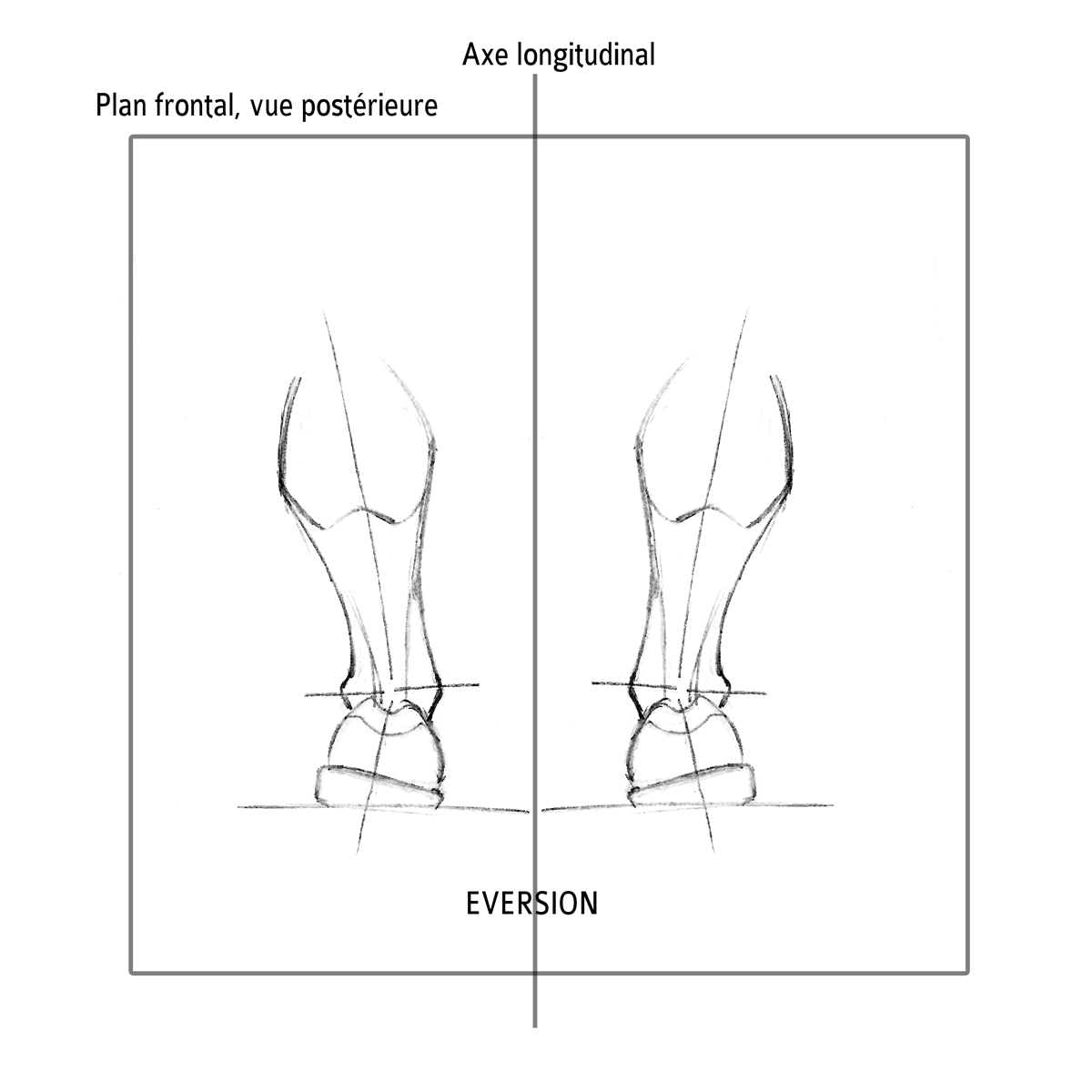
Non Surgical Treatment
If you overpronate, you should talk with a foot and ankle specialist, especially if symptoms have not developed yet. Questions you may want to ask your doctor include what are the best running shoes on the market? Where can I find those shoes? If over-the-counter orthotics don?t work, how long should I wait before contacting you for custom-made orthotics? On my next visit, what type of diagnostic testing should I expect? If I limit the amount of time I spend running, will my overpronation symptoms disappear? What additional treatment options can we try?
Prevention
Exercises to strengthen and stretch supporting muscles will help to keep the bones in proper alignment. Duck stance: Stand with your heels together and feet turned out. Tighten the buttock muscles, slightly tilt your pelvis forwards and try to rotate your legs outwards. You should feel your arches rising while you do this exercise. Calf stretch: Stand facing a wall and place hands on it for support. Lean forwards until stretch is felt in the calves. Hold for 30 seconds. Bend at knees and hold for a further 30 seconds. Repeat 5 times. Golf ball: While drawing your toes upwards towards your shins, roll a golf ball under the foot between 30 and 60 seconds. If you find a painful point, keep rolling the ball on that spot for 10 seconds. Big toe push:
Stand with your ankles in a neutral position (without rolling the foot inwards). Push down with your big toe but do not let the ankle roll inwards or the arch collapse. Hold for 5 seconds. Repeat 10 times. Build up to longer times and fewer repetitions. Ankle strengthener: Place a ball between your foot and a wall. Sitting down and keeping your toes pointed upwards, press the outside of the foot against the ball, as though pushing it into the wall. Hold for 5 seconds and repeat 10 times. Arch strengthener: Stand on one foot on the floor. The movements needed to remain balanced will strengthen the arch. When you are able to balance for 30 seconds, start doing this exercise using a wobble board.
Over-pronation is very common and affects millions of people. To better understand this condition, we'll take a closer look at the 3 most common foot types. An estimated 70% of the population has fallen arches (or a low arch). Only 20% has a normal arch. And 10% have abnormal feet, in other words they either have flat feet or the opposite a high arched foot.
Causes
Over-pronation is very prominent in people who have flexible, flat feet. The framework of the foot begins to collapse, causing the foot to flatten and adding additional stress to other parts of the foot. Therefore over-pronation can often lead to a case of Plantar Fasciitis, Heel Spurs, Metatarsalgia, Post-tib Tendonitis and/or Bunions. There are many causes of flat feet. Obesity, pregnancy or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. People with flat feet often do not experience discomfort immediately, and some never suffer from any discomfort at all. However, when symptoms develop and become painful, walking becomes awkward and causes increased strain on the feet and calves.
Symptoms
When standing, your heels lean inward. When standing, one or both of your knee caps turn inward. Conditions such as a flat feet or bunions may occur. You develop knee pain when you are active or involved in athletics. The knee pain slowly goes away when you rest. You abnormally wear out the soles and heels of your shoes very quickly.
Diagnosis
If you cannot afford to get a proper gait analysis completed, having someone observe you on a treadmill from behind will give you an idea if you are an overpronator. It is possible to tell without observing directly whether you are likely to be an overpronator by looking at your foot arches. Check your foot arch height by standing in water and then on a wet floor or piece of paper which will show your footprint. If your footprints show little to no narrowing in the middle, then you have flat feet or fallen arches. This makes it highly likely that you will overpronate to some degree when running. If you have low or fallen arches, you should get your gait checked to see how much you overpronate, and whether you need to take steps to reduce the level to which you overpronate. Another good test is to have a look at the wear pattern on an old pair of trainers. Overpronators will wear out the outside of the heel and the inside of the toe more quickly than other parts of the shoe. If the wear is quite even, you are likely to have a neutral running gait. Wear primarily down the outside edge means that you are a supinator. When you replace your running shoes you may benefit from shoes for overpronation. Motion control or stability running shoes are usually the best bet to deal with overpronation.
Non Surgical Treatment
If you overpronate, you should talk with a foot and ankle specialist, especially if symptoms have not developed yet. Questions you may want to ask your doctor include what are the best running shoes on the market? Where can I find those shoes? If over-the-counter orthotics don?t work, how long should I wait before contacting you for custom-made orthotics? On my next visit, what type of diagnostic testing should I expect? If I limit the amount of time I spend running, will my overpronation symptoms disappear? What additional treatment options can we try?
Prevention
Exercises to strengthen and stretch supporting muscles will help to keep the bones in proper alignment. Duck stance: Stand with your heels together and feet turned out. Tighten the buttock muscles, slightly tilt your pelvis forwards and try to rotate your legs outwards. You should feel your arches rising while you do this exercise. Calf stretch: Stand facing a wall and place hands on it for support. Lean forwards until stretch is felt in the calves. Hold for 30 seconds. Bend at knees and hold for a further 30 seconds. Repeat 5 times. Golf ball: While drawing your toes upwards towards your shins, roll a golf ball under the foot between 30 and 60 seconds. If you find a painful point, keep rolling the ball on that spot for 10 seconds. Big toe push:
Stand with your ankles in a neutral position (without rolling the foot inwards). Push down with your big toe but do not let the ankle roll inwards or the arch collapse. Hold for 5 seconds. Repeat 10 times. Build up to longer times and fewer repetitions. Ankle strengthener: Place a ball between your foot and a wall. Sitting down and keeping your toes pointed upwards, press the outside of the foot against the ball, as though pushing it into the wall. Hold for 5 seconds and repeat 10 times. Arch strengthener: Stand on one foot on the floor. The movements needed to remain balanced will strengthen the arch. When you are able to balance for 30 seconds, start doing this exercise using a wobble board.
Severs Disease Physical Rehabilitation
Overview
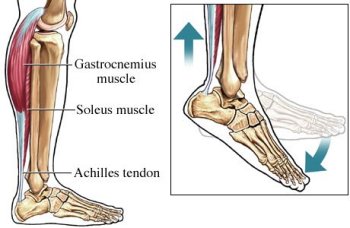
The muscle group at the back of the lower leg is commonly called the calf. The calf comprises of 2 major muscles (known as the gastrocnemius and soleus) both of which insert into the heel bone via the Achilles tendon. In people who have not yet reached skeletal maturity, a growth plate exists where the Achilles tendon inserts into the heel bone. This growth plate is primarily comprised of cartilage. Every time the calf contracts, it pulls on the Achilles tendon which in turn pulls on the heel's growth plate. When this tension is too forceful or repetitive, irritation to the growth plate may occur resulting in pain and sometimes an increased bony prominence at the back of the heel. This condition is called Severs disease. Severs disease is typically seen in children or adolescents during periods of rapid growth. This is because muscles and tendons become tighter as bones become longer. As a result, more tension is placed on the heel's growth plate.
Causes
Sever?s disease is often associated with a growth spurt, when the bones grow but the muscles do not. Therefore the muscles effectively become tighter which results in increased stress at the heel. It may also be related to unusual biomechanics, for instance poor foot posture, muscle tightness or muscle weakness. Overtraining or incorrect training can also play a part. Usually, the cause is a combination of factors.
Symptoms
The pain associated with Sever's disease is usually felt along the back of the heel and becomes worse when running or walking. In some children, the pain is so severe they may limp when walking. One of the diagnostic tests for Sever's disease is the "squeeze test". Squeezing both sides of the heel together will produce immediate discomfort. Many children feel pain immediately upon waking and may have calf muscle stiffness in the morning.
Diagnosis
Low-grade inflammation of the calcaneal apophysis cannot be seen on x-ray. Therefore, although x-rays are often done to rule out bony injuries in children with Sever's disease these x-rays are usually normal. Advanced Sever's disease can be seen on x-ray but usually the problem is treated before it reaches this point. Other diagnostic tests, such as bone scans or MRI's, are not usually required in typical cases of Sever's disease. These, or other tests, may be required to rule out other conditions, such as stress fractures of the calcaneus or other bony abnormalities that can mimic Severs disease.
Non Surgical Treatment
The good news is that the condition doesn?t cause any long-term foot problems. Symptoms typically go away after a few months. The best treatment is simply rest. Your child will need to stop or cut down on sports until the pain gets better. When she's well enough to return to her sport, have her build up her playing time gradually. Your doctor may also recommend ice packs or nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen or naproxen, to relieve the pain. Supportive shoes and inserts that reduce stress on the heel bone. These can help if your child has another foot problem that aggravates Sever?s disease, such as flat feet or high arches. Stretching and strengthening exercises, perhaps with the help of a physical therapist. In severe cases, your child may need a cast so her heel is forced to rest.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
The muscle group at the back of the lower leg is commonly called the calf. The calf comprises of 2 major muscles (known as the gastrocnemius and soleus) both of which insert into the heel bone via the Achilles tendon. In people who have not yet reached skeletal maturity, a growth plate exists where the Achilles tendon inserts into the heel bone. This growth plate is primarily comprised of cartilage. Every time the calf contracts, it pulls on the Achilles tendon which in turn pulls on the heel's growth plate. When this tension is too forceful or repetitive, irritation to the growth plate may occur resulting in pain and sometimes an increased bony prominence at the back of the heel. This condition is called Severs disease. Severs disease is typically seen in children or adolescents during periods of rapid growth. This is because muscles and tendons become tighter as bones become longer. As a result, more tension is placed on the heel's growth plate.
Causes
Sever?s disease is often associated with a growth spurt, when the bones grow but the muscles do not. Therefore the muscles effectively become tighter which results in increased stress at the heel. It may also be related to unusual biomechanics, for instance poor foot posture, muscle tightness or muscle weakness. Overtraining or incorrect training can also play a part. Usually, the cause is a combination of factors.
Symptoms
The pain associated with Sever's disease is usually felt along the back of the heel and becomes worse when running or walking. In some children, the pain is so severe they may limp when walking. One of the diagnostic tests for Sever's disease is the "squeeze test". Squeezing both sides of the heel together will produce immediate discomfort. Many children feel pain immediately upon waking and may have calf muscle stiffness in the morning.
Diagnosis
Low-grade inflammation of the calcaneal apophysis cannot be seen on x-ray. Therefore, although x-rays are often done to rule out bony injuries in children with Sever's disease these x-rays are usually normal. Advanced Sever's disease can be seen on x-ray but usually the problem is treated before it reaches this point. Other diagnostic tests, such as bone scans or MRI's, are not usually required in typical cases of Sever's disease. These, or other tests, may be required to rule out other conditions, such as stress fractures of the calcaneus or other bony abnormalities that can mimic Severs disease.
Non Surgical Treatment
The good news is that the condition doesn?t cause any long-term foot problems. Symptoms typically go away after a few months. The best treatment is simply rest. Your child will need to stop or cut down on sports until the pain gets better. When she's well enough to return to her sport, have her build up her playing time gradually. Your doctor may also recommend ice packs or nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen or naproxen, to relieve the pain. Supportive shoes and inserts that reduce stress on the heel bone. These can help if your child has another foot problem that aggravates Sever?s disease, such as flat feet or high arches. Stretching and strengthening exercises, perhaps with the help of a physical therapist. In severe cases, your child may need a cast so her heel is forced to rest.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Achilles Tendon Rupture Recovery Exercises
Overview
 The Achilles tendon affects your ability to do everything from walking to playing competitive sports. When a patient overstretches his or her Achilles tendon, it can result in a full or partial tear in the tendon, also known as a rupture. In addition to causing a great deal of pain, ruptures can have a profoundly negative impact on your quality of life and prevent you from performing activities you once enjoyed. Because these injuries tend to worsen with time, it?s important to contact a board certified orthopedic surgeon for immediate attention after an Achilles tendon tear.
The Achilles tendon affects your ability to do everything from walking to playing competitive sports. When a patient overstretches his or her Achilles tendon, it can result in a full or partial tear in the tendon, also known as a rupture. In addition to causing a great deal of pain, ruptures can have a profoundly negative impact on your quality of life and prevent you from performing activities you once enjoyed. Because these injuries tend to worsen with time, it?s important to contact a board certified orthopedic surgeon for immediate attention after an Achilles tendon tear.
Causes
There are a number of factors that can increase the risk of an Achilles tendon rupture, which include the following. You?re most likely to rupture your Achilles tendon during sports that involve bursts of jumping, pivoting and running, such as football or tennis. Your Achilles tendon becomes less flexible and less able to absorb repeated stresses, for example of running, as you get older. Small tears can develop in the fibres of the tendon and it may eventually completely tear. There is a very small risk of an Achilles tendon rupture if you have Achilles tendinopathy (also called Achilles tendinitis). This is where your tendon breaks down, which causes pain and stiffness in your Achilles tendon, both when you exercise and afterwards. If you take quinolone antibiotics and corticosteroid medicines, it can increase your risk of an Achilles tendon injury, particularly if you take them together. The exact reasons for this aren't fully understood at present.
Symptoms
Symptoms include a sudden sharp pain in the achilles tendon which is often described as if being physically struck by an object or implement. A loud snapping noise or bang may also be heard at the time. A gap of 4 to 5 cm in the tendon can be felt which may be less obvious later as swelling increases. After a short while the athlete may be able to walk again but without the power to push off with the foot. There will be a significant loss of strength in the injured leg and the patient will be unable to stand on tip toes. There may be considerable swelling around the achilles tendon and a positive result for Thompson's test can help confirm the diagnosis.
Diagnosis
During the physical exam, your doctor will inspect your lower leg for tenderness and swelling. In many cases, doctors can feel a gap in your tendon if it has ruptured completely. The doctor may also ask you to kneel on a chair or lie on your stomach with your feet hanging over the end of the exam table. He or she may then squeeze your calf muscle to see if your foot will automatically flex. If it doesn't, you probably have ruptured your Achilles tendon. If there's a question about the extent of your Achilles tendon injury, whether it's completely or only partially ruptured, your doctor may order an ultrasound or MRI scan. These painless procedures create images of the tissues of your body.
Non Surgical Treatment
As debilitating as they can be, the good news is that minor to moderate Achilles tendon injuries should heal on their own. You just need to give them time. To speed the healing, you can try the following. Rest your leg. Avoid putting weight on your leg as best you can. You may need crutches. Ice your leg. To reduce pain and swelling, ice your injury for 20 to 30 minutes, every three to four hours for two to three days, or until the pain is gone. Compress your leg. Use an elastic bandage around the lower leg and ankle to keep down swelling. Elevate your leg. Prop you leg up on a pillow when you're sitting or lying down. Take anti-inflammatory painkillers. Nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen (Advil, Motrin) and naproxen (Aleve) will help with pain and swelling. However, these drugs have side effects, such as an increased risk of bleeding and ulcers. They should be used only occasionally unless your health care provider says otherwise and should be taken with food. Check with your doctor before taking these if you have any allergies, medical problems or take any other medication. Use a heel lift. Your health care provider may recommend that you wear an insert in your shoe while you recover. It will help protect your Achilles tendon from further stretching. Practice stretching and strengthening exercises as recommended by your health care provider. Usually, these techniques will do the trick. But in severe cases of Achilles tendon injury, you may need a cast for six to 10 weeks or even surgery to repair the tendon or remove excess tissue. 
Surgical Treatment
This injury is often treated surgically. Surgical care adds the risks of surgery, there are for you to view. After the surgery, the cast and aftercare is typically as follows. A below-knee cast (from just below the knee to the tips of the toes) is applied. The initial cast may be applied with your foot positioned in a downward direction to allow the ends of the tendon to lie closer together for initial healing. You may be brought back in 2-3 week intervals until the foot can be positioned at 90 degrees to the leg in the cast. The first 6 weeks in the cast are typically non-weight bearing with crutches or other suitable device to assist with the non-weight bearing requirement. After 6 weeks in the non-removable cast, a removable walking cast is started. The removable walking cast can be removed for therapy, sleeping and bathing. The period in the removable walking cast may need to last for an additional 2-6 weeks. Your doctor will review a home physical therapy program with you (more on this program later) that will typically start not long after your non-removable cast is removed. Your doctor may also refer you for formal physical therapy appointments. Typically, weight bearing exercise activities are kept restricted for at least 4 months or more. Swimming or stationary cycling activities may be allowed sooner. Complete healing may take 12 months or more.